Kefah Mokbel
Ductal carcinoma in situ (DCIS) is a heterogeneous disease characterized by noninvasive clonal proliferation of malignant epithelial cells arising from the mammary ducts and terminal ductal-lobular units. Its reported incidence is rising due to the wide adoption of screening mammography and magnetic resonance imaging (MRI). The combination of nuclear grade and presence of necrosis is currently the best predictor of biological behavior. DCIS should be managed in the context of a multidisciplinary team. Local control depends upon adequate surgical clearance with margins of
at least 2mm. Sentinel lymph node biopsy (SLNB) is not routinely indicated and should be reserved for those with concurrent or recurrent invasive disease. SLNB can be considered in patients undergoing mastectomy (MX) and those with risk factors for invasion such as palpability, comedo morphology, necrosis or recurrent disease. Radiotherapy (RT) following breast conserving surgery (BCS) significantly reduces local recurrence (LR), particularly in those at high-risk. There remains a lack of level-1 evidence supporting the omission of adjuvant RT in selected low risk cases. Large, multi-centric or recurrent lesions (particularly in cases of prior RT) should be treated by MX with the opportunity for immediate reconstruction. Adjuvant Tamoxifen may reduce the risk of LR in selected cases with hormone sensitive disease. Further research is required to determine the role of contemporary RT regimes and endocrine therapies. Biological profiling and molecular analysis represent an opportunity to improve our understanding of the tumour biology of this condition and rationalise its treatment. Reliable identification of low-risk lesions could allow treatment to be less radical or safely omitted.
Share this article
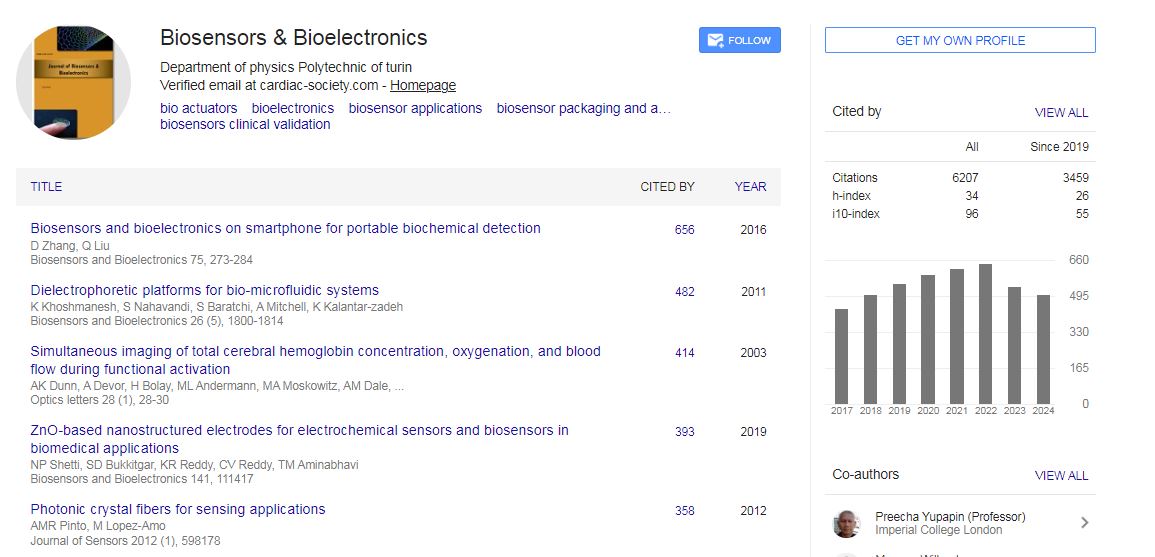
Biosensors & Bioelectronics received 6207 citations as per Google Scholar report